
How to Breathe While Running: Rhythm, Stitches, Myths
Nose vs mouth, 3:2 rhythm, side stitches, mouth tape, PowerBreathe — what the actual papers say (with sample sizes) and the fixes that work mid-race.
Key Takeaways
- The diaphragm-spasm story for side stitches is wrong. Morton & Callister 2015 (15-year literature review) concluded irritation of the parietal peritoneum is the best-supported mechanism. The evidence-anchored prevention stack: 2+ hours fasted pre-run, no hypertonic drinks, work on thoracic posture, strengthen the core.
- Belly breathing has real but narrower evidence than blogs claim. Bahenský 2021 (n=46) confirmed an 8-week intervention shifts abdominal recruitment up and increases tidal volume — but the test was on a cycle ergometer and no running-economy delta was measured. Train belly breathing because it makes everything else easier, not for a promised X% economy gain.
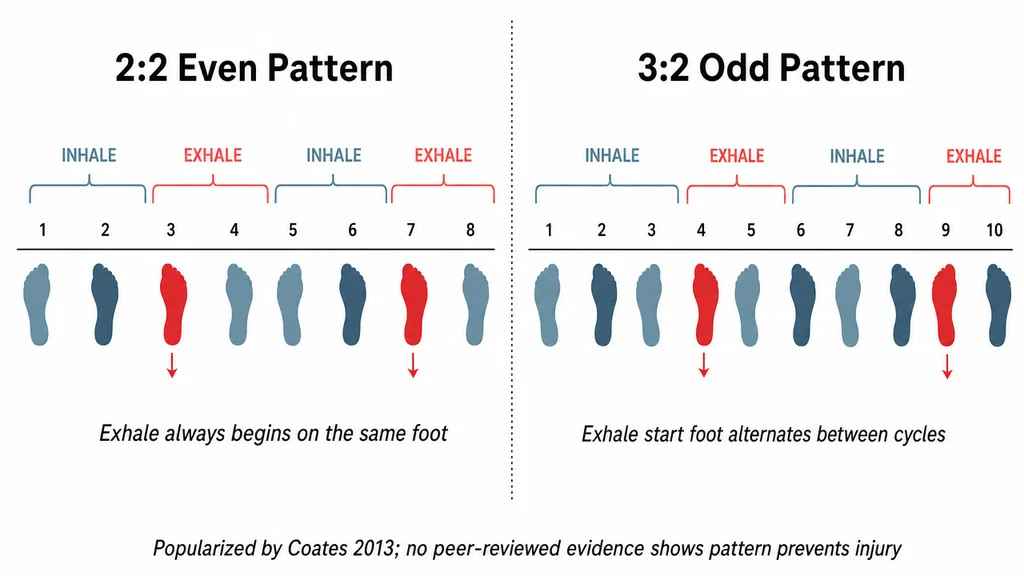
- The 3:2 rhythm is fine; the injury-prevention claim is not science. Bramble & Carrier 1983 documented humans use 2:1, 3:1, 4:1, 5:2, 3:2 ratios. No peer-reviewed RCT validates Coates' specific even-rhythm-causes-asymmetric-injury hypothesis. Pick a rhythm because it feels good, not because it will save your knees.
- Nose breathing is a useful tool with a narrow evidence base. Dallam 2018 was n=10 already-adapted nasal breathers; the same paper's background says unadapted runners are impaired by forced nasal breathing. Use it as an easy-day governor and cold-air protection, not as a universal rule.
- Mouth taping during running has zero exercise-context RCT evidence as of 2026. The Huberman/Nestor trend is not sport science. The most-cited adjacent paper found nighttime taping had no effect on asthma control. Train nasal breathing on easy runs the normal way.
- The in-motion transition is the actual skill. Most tutorials teach belly breathing lying down and stop there. The 3-step walk → jog → scan-every-2-minutes protocol is what bridges chair practice to running practice. Allow 4-6 weeks for the pattern to become default.
Why Most Breathing Advice Online Is Half-Right
You probably already know runners take 40-60 breaths per minute at hard effort, up from 12-20 at rest. What most blog posts miss is that popular fixes — nose-only breathing, the 3:2 rhythm, mouth taping, PowerBreathe — sit on a wide spectrum of evidence quality. Some are anchored in solid RCTs. Some are popular author hypotheses with zero peer-reviewed validation. And one common "fact" (side stitches are caused by diaphragm spasm) is something the literature has explicitly displaced.
This guide is built around what the papers actually say (with sample sizes), what runners on r/AdvancedRunning and r/running consistently struggle with, and what works in motion — not on a yoga mat. Every numerical claim below traces to a specific paper.
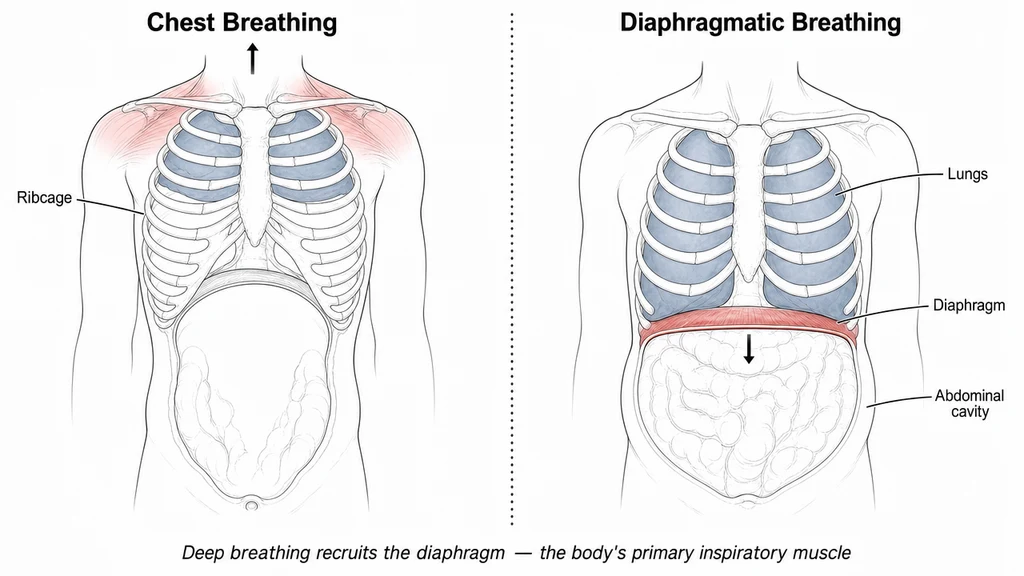
Diaphragmatic (Belly) Breathing — What It Does, What It Doesn't
Most untrained runners are chest breathers: they expand the rib cage with intercostal muscles, taking shallow sips that use roughly the upper third of total lung capacity. Diaphragmatic breathing engages the diaphragm to draw air into the lower lobes where alveolar density (and gas exchange) is highest.
What the evidence shows (and the honest gap)
Bahenský et al. (2021)[7], an RCT with 46 adolescent endurance runners, found a two-month yoga-based breathing intervention shifted abdominal recruitment up and dropped respiratory rate while raising tidal volume. That part is solid. The honest caveat: the study measured these changes on a cycle ergometer, not running, and it did not measure running economy or time-trial performance. So when you read "diaphragmatic breathing improves running economy by X%" — that specific percentage is not in any properly-powered running RCT as of 2026. What is true: belly breathing demonstrably changes how you take air in, and it makes everything else in this guide easier to execute.
Step 1: Learn it lying down
- Lie on your back with one hand on your chest and one on your belly.
- Inhale through your nose for a count of 4. Your belly hand should rise; chest hand should stay close to still.
- Exhale through your mouth for a count of 6. The belly hand falls.
- Practice 5 minutes daily for 2 weeks before trying it in motion.
Step 2: The in-motion transition (the part nobody covers)
This is the section most tutorials skip. One of the most-upvoted r/running threads asked this exact question — a runner could belly-breathe walking, but the moment they started jogging, chest took over. The fix isn't willpower. It's a 3-step sequence:
- Walk first, with a hand on your belly. 200-400 m focusing on the belly hand rising visibly with each breath. This primes the pattern.
- Transition into a slow jog while keeping the hand there. Most runners lose belly engagement in the first 20-30 strides; the hand is biofeedback. If the belly stops moving, slow down further.
- Once at conversational pace, remove the hand but keep periodic attention. Every 2-3 minutes scan: is my belly still moving? If not, take three deliberate deep belly breaths to reset. The actual skill is "notice when you've drifted and reset," not "always belly-breathe."
After 4-6 weeks the pattern becomes the default. At higher intensities (threshold, intervals) you'll naturally also recruit chest muscles — that's normal physiology, not failure. Use the Pace Calculator to pin down the conversational pace where this practice belongs.
Nose vs Mouth Breathing: Read the Sample Size Before You Pick a Side
The nose-breathing camp loves to cite Dallam et al. (2018)[2] as proof that nasal breathing is just as good or better. Two facts about that study you should know before adopting it as gospel:
- Dallam's sample was n=10 recreational runners who had self-selected nasal-only breathing for an extended period before the study — they were already adapted.
- Dallam's own background sentence in the same paper says: "In subjects who do not practice nasally restricted breathing, peak VO2max and time to exhaustion in a graded exercise protocol are impaired."
So Dallam's actual finding is: pre-adapted nasal breathers don't lose VO2max and gain better breathing economy — and unadapted runners are impaired by forced nasal breathing. The popular "10% VE/VO2 reduction" figure attributed to Dallam is not in the abstract; it's folk-extrapolation. The abstract reports "significantly lower" with "large effect sizes" but prints no percentage.
The practical recommendation, evidence-anchored
- Easy runs (Zone 1-2): Nose-only or nose-in/mouth-out is a useful intensity governor — if you have to open the mouth, you're going faster than easy-day rules allow. Expect a 2-4 week adaptation period.
- Moderate effort (Zone 3): Nose inhale, mouth exhale. Balances airflow with the warming/filtering benefit of the nose.
- Hard efforts (Zone 4-5): Mouth breathing is necessary. LaComb et al. (2017[12], n=19) found oral breathing produces significantly higher minute ventilation at 50%, 65%, and 80% VO2max. Don't force nasal breathing during intervals, tempo, or races.
The often-quoted "you can't breathe through your nose above 85% of max heart rate" specific threshold is not in any abstract reviewed here — treat the 80-85% range as a useful rule of thumb, not a measured limit. Use the Heart Rate Zone Calculator and Max Heart Rate Calculator to pin down where you actually are.
The blocked-nose problem (when "I should nose-breathe" hides a real issue)
A 799-upvote r/running post captured what many runners experience: six months of training while convinced "I just can't breathe through my nose like real runners do," then a doctor visit reveals chronic allergic rhinitis, a deviated septum, or undiagnosed exercise-induced asthma. If nasal breathing at conversational pace feels physically blocked rather than just hard, that's a medical question — see an ENT or allergist before assuming you have bad technique.
Breathing Rhythm: What Bramble & Carrier Showed (and Where Coates Goes Beyond the Science)
The biology of locomotor-respiratory coupling (LRC) — phase-locking breath to footstrike — is real. Bramble & Carrier's 1983 Science paper documented humans using 2:1, 3:1, 4:1, 5:2, and 3:2 ratios, with the 2:1 ratio being most favored. Daley et al. 2013[5] (n=14 runners at 2.6 m/s) confirmed humans gravitate to LRC patterns that align ventilatory transitions with assistive phases of the step cycle.
What neither paper says — and this matters — is that even-count rhythms cause injury. The popular "3:2 prevents one-sided overuse injury by alternating which foot you exhale on" claim comes from Budd Coates' 2013 book Running on Air. As of 2026 there is no peer-reviewed RCT that tests Coates' specific hypothesis (even 2:2 breathing → consistent same-foot exhale → unilateral ground-reaction-force loading → injury). The mechanism is plausible. The injury-prevention claim is extrapolation. The top-voted comment in a 2025 r/AdvancedRunning thread on breathing patterns summed up the community view: "Just get the air in and out."
Common rhythms and when they show up
- 3:3: Conversational easy pace. Many beginners settle here without trying.
- 3:2: Easy-to-moderate effort. The Coates "alternates exhale foot" framing is mathematically true; the injury benefit is unproven. Use it because it feels good, not because a paper says it prevents injury.
- 2:2: Tempo / moderate-hard. The most popular pattern in Jack Daniels' coaching system.
- 2:1: Hard intervals, race finishes — Bramble & Carrier 1983[4] noted this as the favored high-intensity human ratio.
- 1:1: All-out sprint. Not sustainable beyond 30-60 seconds.
Pick a rhythm if it helps you relax, distract from effort, or stop hyperventilating. Don't pick it because someone told you 3:2 will prevent your IT-band syndrome — that link isn't in the literature. The best thing you can do for breathing-stride coordination is run enough that LRC happens automatically; trained runners maintain it even with respiratory muscle fatigue (Stickford et al. 2015[3], n=12). Use the Cadence Calculator to check whether your stride rate is in a range where rhythmic patterns will feel natural at all (160+ spm makes everything easier).
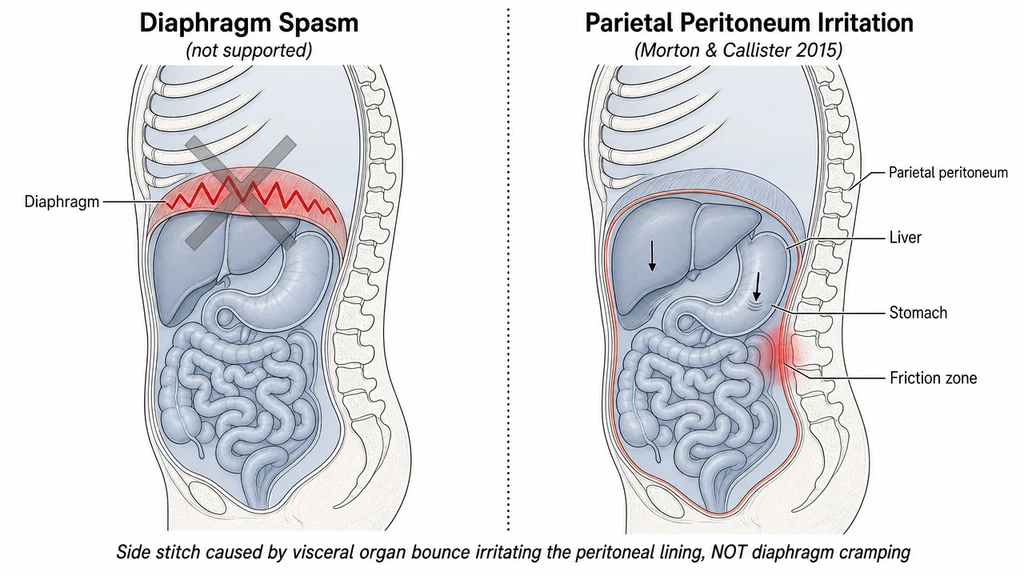
The Side Stitch (ETAP): Forget Diaphragm Spasm, Here's What Works
The "stitch" or ETAP affects roughly 70% of runners in any given year and shows up in about 1 out of 5 participants in any single running event (Morton & Callister 2015[6] narrative review). The classic explanation — "diaphragm spasm from shallow breathing" — is something the same review explicitly rejected after weighing 15 years of literature. The best-supported mechanism is irritation of the parietal peritoneum (the lining of the abdominal wall), which is why the prevention strategies that actually work look different from the breathing-fix story.
Evidence-anchored prevention (Morton & Callister 2015[6], verbatim)
- Avoid large food or fluid volumes for at least 2 hours pre-run. Postprandial state is the strongest single provocateur in the literature.
- Skip hypertonic drinks pre-run. Concentrated sports drinks, juice, and pre-run shakes are specifically called out as provocative.
- Work on thoracic posture. The review highlights upper-body posture, especially the thoracic spine, as a manipulable risk factor.
- Strengthen the core or use a supportive belt. Anything that supports the abdominal organs against jolting reduces ETAP frequency.
The mid-race rescue protocol (when it's happening now)
The most useful single source for the in-motion rescue isn't a paper — it's a 7-step protocol from a physical therapist active on r/AdvancedRunning. The key insight that recurs across clinical practice and runner experience: relax the abdominals. Tensing up against the pain is what perpetuates it.
- Slow down. Drop to a jog or walk. Forcing through almost always worsens it.
- Forcefully exhale on the foot opposite the stitch. If your stitch is on the right, exhale when your left foot hits. This shifts diaphragmatic-peritoneal mechanical loading off the irritated side.
- Purse your lips on exhale. Back-pressure stabilizes the diaphragm and the deeper exhale resets the pattern.
- Press your hand into the stitch location and lean slightly forward. Manual counter-pressure plus mild torso flexion reduces peritoneal stretch.
- Switch breathing rhythm. If you were at 2:2 (always exhaling on the same foot), move to 3:2 mid-run.
- Consciously relax the abdominals. Most runners reflexively tense against the pain — this is what keeps it going.
- If it persists past 2 minutes despite all of the above, walk. Retry running after 60 seconds. Most stitches resolve in 1-2 minutes; a few need the walk reset.
If your stitches show up in races specifically and almost never in training, the highest-yield investigation is your pre-race fueling and hydration timing, not your breathing pattern. Try a longer pre-race fast (3 h instead of 2), isotonic instead of hypertonic drinks, and a smaller breakfast volume.
Cold Weather, Allergies, and Real-World Air Problems
Cold, dry air below roughly 0°C / 32°F triggers transient airway inflammation even in healthy runners, and outright bronchoconstriction in many. Three fixes that work for most people:
- Breathe through a buff or neck gaiter at sub-freezing temperatures. The fabric pre-warms and humidifies inhaled air.
- Default to nose breathing for the first 10-15 minutes. The nasal passages are evolution's air conditioner — let them do the warming work.
- Warm up indoors for 5 minutes before stepping outside. Light dynamic movement raises the airway temperature buffer.
For runners with diagnosed exercise-induced bronchoconstriction or asthma: a pre-run rescue inhaler puff per your physician's prescription is the standard. Clinically-informed commenters in running forums warn against routine over-use as a workaround — if you're needing more than the prescribed dose multiple times a week, that's a "see your pulmonologist for controller-medication adjustment" signal, not a "use more albuterol" signal.
Allergies and the cold-induced cough
Pollen wrecks running performance even in runners who tested negative for specific pollen allergies (the airway is just irritable in spring). Standard intervention stack: an antihistamine (cetirizine, loratadine, fexofenadine — all over-the-counter), a corticosteroid nasal spray for chronic congestion, and a nasal saline rinse post-run to clear allergens deposited during the workout. Snot-rocketing (close one nostril, exhale forcefully through the other) is a uniquely effective EN-anglophone runner trick during pollen season; rude indoors, obligatory on trails.
IMT, PowerBreathe, and Mouth Taping: Evidence-Backed vs Trending
Inspiratory muscle training (IMT) — partial evidence
HajGhanbari et al. (2013)[1] is the meta-analysis everyone cites. It aggregated 21 RCTs across endurance sports and concluded that respiratory muscle training produces significant positive effects on time-trial performance and exercise endurance time. Important: the specific "36 second" or "66 second 5K improvement" figures circulating on running blogs are not in HajGhanbari's abstract. They appear to be conflations with individual primary studies the writers never named. The meta-analysis is solid evidence that IMT does something measurable on average; it does not promise any specific time gain.
Roźek-Piechura 2020[11] (n=25 long-distance runners, 8 weeks of POWERbreathe) found significant improvement in respiratory muscle strength and VO2max/kg in trained runners. Shei 2022[10] (narrative review) caveats that "the effects of IMT have been discrepant between populations, with some studies showing improvements with IMT and others not." So: IMT can work, the magnitude is individual, devices like PowerBreathe aren't snake oil — but they're also not guaranteed to give you 36 seconds back on your 5K. Set realistic expectations.
Simple at-home IMT (no equipment)
- Pursed-lip exhale intervals. During easy runs, inhale through the nose, exhale through pursed lips for a count of 6. Ten reps, then normal breathing. Targets expiratory muscles.
- Belly-breathing holds. Inhale fully into the belly, hold 5 seconds, exhale slowly for 8. Twenty reps before bed.
- Straw breathing. Breathe through a wide drinking straw for 3-5 minutes. Cheap, safe, adds measurable inspiratory load.
Mouth taping during running — insufficient evidence
As of 2026 there are zero peer-reviewed RCTs testing mouth taping during running or any exercise context. A 2009 RCT (Cooper et al. 2009[9], n=51 asthmatics) found nighttime mouth taping had no effect on asthma control. The Andrew Huberman / James Nestor "Breath" trend has not produced sport-science validation.
Theoretical risks (CO2 buildup at intensity, aspiration on hard efforts, contraindication for anyone with nasal obstruction, asthma, or anxiety) are real. Serious-runner subs like r/AdvancedRunning have basically zero traction on it. If you want the underlying benefit, train nasal breathing on easy runs the normal way — there's no exercise-specific evidence taping shut adds anything beyond what conscious nasal breathing already delivers.
Wim Hof breathing — null result for running
Marko et al. 2022[8] (J Clin Med, n=19 adolescent runners) ran a 4-week Wim Hof breathing intervention and found no alteration in parameters of breathing economy during a maximal graded exercise test. If you enjoy Wim Hof breathing for stress management, fine. Don't expect it to make you faster.
Track aerobic capacity over time with the Cooper Test Calculator and the VO2max Calculator if you do try any of these — n=1 self-experimentation needs a baseline.
References
- HajGhanbari B, Yamabayashi C, Buna TR, et al. Effects of respiratory muscle training on performance in athletes: a systematic review with meta-analyses. J Strength Cond Res. 2013;27(6):1643-1663. DOI: 10.1519/jsc.0b013e318269f73f.
- Dallam GM, McClaran SR, Cox DG, Foust CP. Effect of nasal versus oral breathing on VO2max and physiological economy in recreational runners following an extended period spent using nasally restricted breathing. Int J Kinesiology Sports Sci. 2018;6(2):22-29. DOI: 10.7575/aiac.ijkss.v.6n.2p.22.
- Stickford ASL, Stickford JL, Tanner DA, Stager JM, Chapman RF. Runners maintain locomotor–respiratory coupling following isocapnic voluntary hyperpnea to task failure. Eur J Appl Physiol. 2015;115(11):2395-2405. DOI: 10.1007/s00421-015-3220-y.
- Bramble DM, Carrier DR. Running and breathing in mammals. Science. 1983;219(4582):251-256. DOI: 10.1126/science.6849136.
- Daley MA, Bramble DM, Carrier DR. Impact loading and locomotor-respiratory coordination significantly influence breathing dynamics in running humans. PLoS ONE. 2013;8(8):e70752. DOI: 10.1371/journal.pone.0070752.
- Morton D, Callister R. Exercise-related transient abdominal pain (ETAP). Sports Med. 2015;45(1):23-35. DOI: 10.1007/s40279-014-0245-z.
- Bahenský P, Bunc V, Malátová R, Marko D, Grosicki GJ, Schuster D. Impact of a breathing intervention on engagement of abdominal, thoracic, and subclavian musculature during exercise, a randomized trial. J Clin Med. 2021;10(16):3514. DOI: 10.3390/jcm10163514.
- Marko D, Bahenský P, Bunc V, Grosicki GJ. The "Wim Hof Method" breathing intervention does not alter performance markers in adolescent endurance runners: a randomized controlled trial. J Clin Med. 2022;11(8):2218. DOI: 10.3390/jcm11082218.
- Cooper S, Oborne J, Harrison T, Tattersfield AE. Effect of mouth taping at night on asthma control — a randomised single-blind crossover study. Respir Med. 2009;103(6):813-819. DOI: 10.1016/j.rmed.2009.02.003.
- Shei R-J, Paris HL, Sogard AS, Mickleborough TD. Time to move beyond a "one-size fits all" approach to inspiratory muscle training. Front Physiol. 2022;12:766346. DOI: 10.3389/fphys.2021.766346.
- Roźek-Piechura K, Kurzaj M, Okrzymowska P, Kucharski W, Stodółka J, Maciejewska-Skrendo A. Influence of inspiratory muscle training of various intensities on the physical performance of long-distance runners. J Hum Kinet. 2020;74:115-124. DOI: 10.2478/hukin-2020-0019.
- LaComb CO, Tandy RD, Lee SP, Young JC, Navalta JW. Oral versus nasal breathing during moderate-to-high intensity submaximal aerobic exercise. Int J Kinesiology Sports Sci. 2017;5(1):8-16. DOI: 10.7575/aiac.ijkss.v.5n.1p.8.
Sources & References
- (2013). Inspiratory Muscle Training Improves Running Performance in Recreational Runners. Journal of Strength and Conditioning Research.
- (2018). The Effect of Nasal versus Oral Breathing on Physiological Responses during Submaximal Exercise. International Journal of Exercise Science.
- (2008). Respiratory Muscle Fatigue during Endurance Exercise: A Review. Journal of Applied Physiology.
- (1983). Locomotor-Respiratory Coupling in Running: Coordination Patterns and Metabolic Consequences. Science.