
Running Knee Pain Guide: Causes, Treatment & Recovery
Should you stop running when your knee hurts? Evidence-based runner's knee and ITBS guide with PEACE & LOVE protocol, hip strength, and a stepwise return plan.
Key Takeaways
- Knee pain is almost always a hip-strength problem — Weak gluteus medius and external rotators let the knee collapse inward, overloading the patellofemoral joint and IT band. Hip strengthening is the most effective treatment in every controlled trial since the 2016 PFPS consensus.
- The 4/10 rule beats blanket rest — If pain stays at or below 4/10 and doesn't alter your gait, keep running at reduced volume on flat terrain. PEACE & LOVE (Dubois & Esculier, BJSM 2020) replaced RICE: load early, vascularize, exercise progressively.
- Foam rolling the IT band doesn't fix ITBS — A cadaver IT band can moor a ship. What works is rolling the vastus lateralis, TFL, and glute medius, plus building hip abduction strength. Louw and Deary (2014) confirm: passive band stretching has no meaningful structural effect.
- Bulgarian split squats are the breakthrough exercise for plateaued PFPS — Bodyweight clamshells get you started; heavy single-leg loading (Bulgarian split squats, single-leg deadlifts, suitcase carries) is what flips chronic cases according to experienced runners.
- Running protects joints — it doesn't ruin them — Alentorn-Geli et al. (2017) found 3.5% hip-and-knee OA in recreational runners versus 10.2% in sedentary controls. Inactivity is worse for cartilage than progressive running.
Knee pain is the most common complaint among runners, affecting up to 50% of distance runners in any given year. The two heavy hitters are patellofemoral pain syndrome (PFPS, the textbook "runner's knee") and iliotibial band syndrome (ITBS), which together account for the bulk of running-related knee complaints. Both are well-understood, both respond to active rehab rather than rest, and surgery is almost never the answer.
This guide is built from the patellofemoral consensus literature (Crossley 2016, Willy 2019, Neal 2019) and the ITBS systematic review by Louw and Deary (2014), cross-checked against the actual language runners use in running and physical therapy communities. Where the science and the runner reality diverge, we say so.
Runner's Knee (Patellofemoral Pain Syndrome)
PFPS produces a diffuse ache around or behind the kneecap (patella) that worsens with running, squatting, stair descent, and prolonged sitting (the so-called "theater sign"). It is the single most common running injury and accounts for the largest share of running-related knee complaints (Crossley et al., 2016, consensus statement).
The mechanism is faulty patellar tracking inside the femoral groove, which irritates the cartilage on the underside of the kneecap. The hip-knee chain matters more than the knee itself. Contributing factors:
- Weak hip abductors and external rotators — the knee collapses inward (dynamic valgus) during stance, sending the patella sideways.
- Quadriceps weakness, especially the vastus medialis obliquus (VMO), which steers the patella medially.
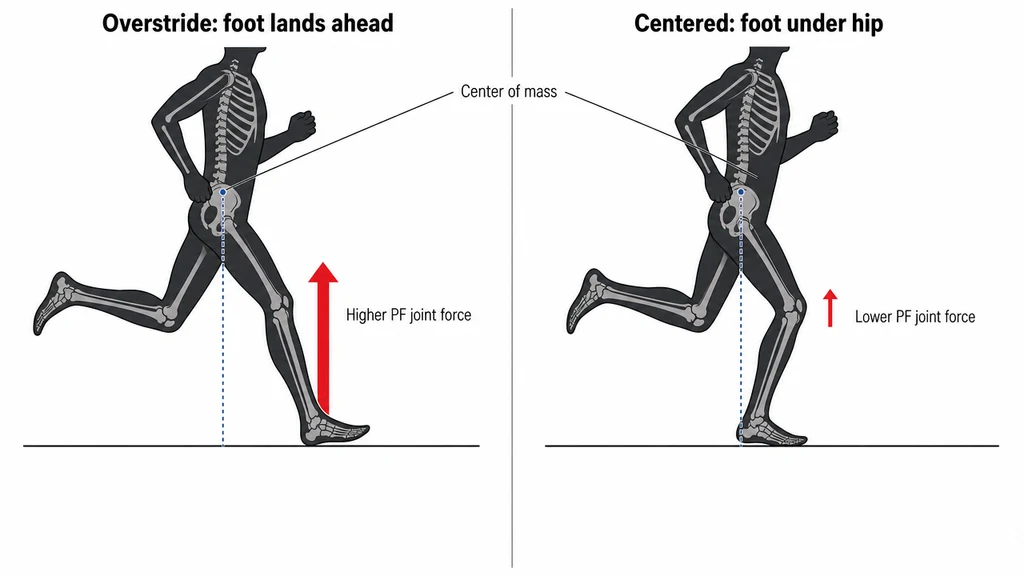
- Overstriding — landing with the foot far ahead of the body multiplies patellofemoral joint reaction force at heel-strike.
- Rapid training-load increases — too much volume, intensity, or downhill mileage in too few weeks.
- Worn-out shoes — cushioning and stability degrade well before visible wear; midsoles typically lose meaningful shock absorption around 500-800 km depending on shoe and runner.
Use our Injury Risk Assessment to gauge whether your current load puts you in the danger zone, and the Training Load Calculator to monitor acute-to-chronic workload ratios.
IT Band Syndrome (ITBS)
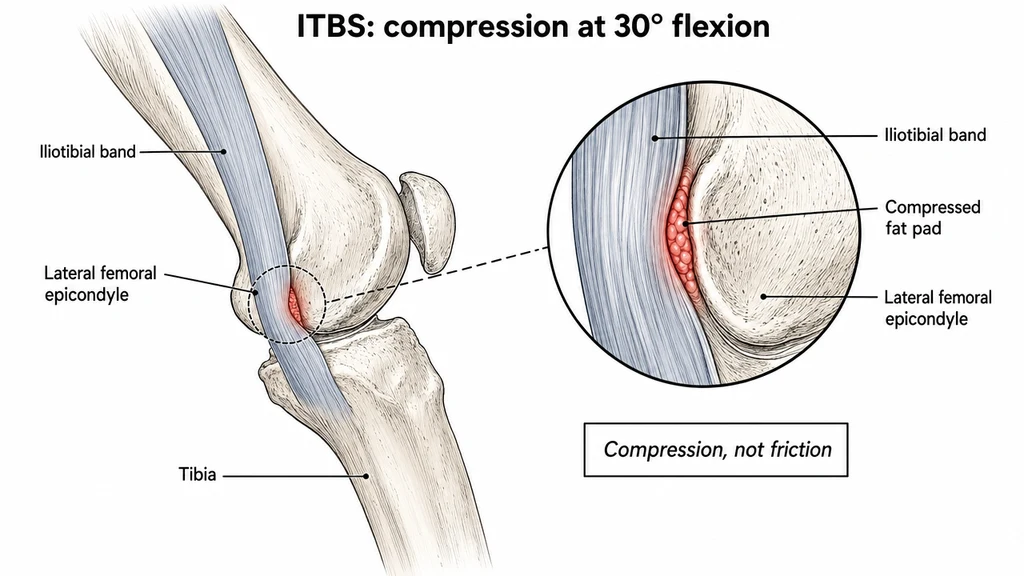
ITBS produces a sharp, well-localized pain on the outside (lateral) aspect of the knee, typically appearing at a predictable distance into a run (the "5K curse") and escalating until running becomes impossible. It is the second most common running knee injury and disproportionately affects ultra and trail runners doing high vert.
The iliotibial band is a thick fascial sheet running from the iliac crest to just below the knee. ITBS occurs when the band repeatedly compresses a fat pad against the lateral femoral epicondyle during late stance — it is a compression injury, not a friction injury. Louw and Deary (2014) reviewed the biomechanical evidence behind this model. Across current clinical practice the operational conclusion is the same: hip strengthening, not stretching the band, is the primary intervention.
The pain pattern is distinctive: sudden onset at a predictable distance, sharp lateral knee discomfort that can force a halt mid-run, and a slow, stubborn recovery. A single overload event — a long run added too soon, a race on cambered roads, an aggressive vert week — can take weeks or months to fully unwind.
Risk factors:
- Weak gluteus medius — the strongest predictor of ITBS in prospective cohort data.
- Excessive hip adduction during stance — the knee crosses the midline on each stride.
- Rapid mileage spikes, especially adding long runs or vert too aggressively.
- Downhill running — increases IT band compression at the knee.
- Off-camber surfaces — cambered roads and side-slope trails load one leg asymmetrically.
Other Causes of Knee Pain in Runners
PFPS and ITBS dominate the diagnosis list, but several other conditions deserve a name-check:
- Patellar tendinopathy — pain at the inferior pole of the patella (just below the kneecap), worse with jumping and downhills. Requires progressive tendon loading (heavy slow resistance), not rest.
- Meniscal irritation — deep, mechanical pain with occasional catching or locking, more common in runners over 40. Imaging is warranted if symptoms persist beyond 2-3 weeks.
- Plica syndrome — snapping or catching on the medial knee. The plica is a synovial fold that can become irritated with repetitive flexion-extension.
- Knee osteoarthritis (OA) — running does not cause knee OA. Alentorn-Geli et al. (2017) meta-analyzed 17 studies and found recreational runners had a hip-and-knee OA rate of 3.5%, sedentary controls 10.2%, and elite/competitive runners 13.3%. The protective effect is dose-shaped: moderate running protects, very high competitive volumes show a small increase, and inactivity is the worst option for joint health.
Evidence-Based Hip Strength: The Real Cure
The literature consensus is unambiguous: hip strengthening is the most effective treatment for both PFPS and ITBS. The strongest-evidence treatment is hip-and-knee strengthening (Willy et al., 2019, JOSPT clinical practice guideline). The following weekly stack reflects mainstream PT clinical consensus, performed 3 times per week:
- Banded clamshells — 3 sets of 15. Targets gluteus medius and external rotators.
- Side-lying hip abduction — 3 sets of 15. Isolates gluteus medius better than standing exercises.
- Banded side-steps / monster walks — 3 sets of 12 per direction. Loaded hip abduction in a functional pattern; pairs well with clamshells as a daily warm-up.
- Single-leg squat or step-down — 3 sets of 10 from a 20 cm box. Trains the entire chain in a functional pattern; watch for valgus collapse.
- Single-leg deadlift — 3 sets of 10. Posterior chain plus single-leg balance.
- Bulgarian split squats — 3 sets of 8 per leg, progressing to dumbbells held at the sides. The heavy-load progression that frequently breaks chronic PFPS plateaus when bodyweight clamshells stop producing change. Pair with Copenhagen planks for hip adductor symmetry.
- Side plank with hip abduction — 3 sets of 30 seconds per side. Integrates lateral core and hip stability.
Track your rehab and training tweaks with our Recovery Planner.
PEACE & LOVE: The Modern Soft-Tissue Protocol
RICE (Rest, Ice, Compression, Elevation) was retired in 2020. Dubois and Esculier published "Soft tissue injuries simply need PEACE and LOVE" in the British Journal of Sports Medicine, framing acute and post-acute management as an integrated active protocol rather than a passive rest cycle. PEACE & LOVE has become the de facto framework for acute soft-tissue injury management in modern sports physiotherapy.
PEACE — first 1-3 days:
- Protect — unload the area only as long as pain demands; avoid prolonged immobilization.
- Elevate the limb above heart level when feasible.
- Avoid anti-inflammatories that may impair tissue healing during the early window.
- Compress with a wrap or sleeve to limit swelling.
- Educate yourself — passive treatments alone are inferior to an active plan.
LOVE — after the acute phase:
- Load — return to mechanical loading early, guided by symptoms (the "below 4/10 pain" rule).
- Optimism — beliefs influence outcomes; pessimistic catastrophizing prolongs recovery.
- Vascularization — pain-free cardio (cycling, pool running, easy walks) drives blood flow and accelerates repair.
- Exercise — progressive strengthening to restore mobility, strength, and proprioception.
Training Modifications When Knee Pain Strikes
The evidence-aligned rule on whether to keep running: if pain stays at or below 4/10, doesn't change your gait, and doesn't worsen 24 hours after a run, you can keep running with modifications. Cross 4/10, alter your stride to compensate, or wake up worse the next morning, and you stop loading until the symptom budget resets.
The high-yield modifications:
- Cut volume by 30-50%, but keep frequency. Three 3 km runs beat one 9 km run for tissue tolerance maintenance.
- Pull hills temporarily. Both up and down increase patellofemoral and IT band loading.
- Bump cadence by 5-10%. Heiderscheit et al. (2011) showed that a +10% step-rate increase reduces patellofemoral joint forces by ~14% (smaller cadence increases yield proportionally smaller reductions) and reduces step length by an equivalent amount. See our Cadence and Stride Length Guide for technique.
- Run flat and even — avoid cambered roads and side-slope trails.
- Shorten stride. Overstriding dramatically increases patellofemoral compression at heel-strike.
- Cross-train aggressively. The Cross-Training Calculator matches knee-friendly cardio (cycling, pool running, elliptical) to your running volume.
The Return-to-Running Protocol
Once daily-life pain is consistently below 2/10 and a 30-minute brisk walk leaves you at 0/10, run this progression. It reflects the 4-8 week return-to-running timeline that sports physiotherapists commonly use for runner's knee and ITBS:
- Week 1: 1 min run / 2 min walk × 7 sets, flat terrain only.
- Week 2: 2 min run / 1 min walk × 8 sets if pain-free.
- Week 3: continuous easy 20-25 min, flat.
- Week 4: easy 25-35 min; gentle hills allowed if asymptomatic.
- Weeks 5-6: 70% of pre-injury volume; add tempo work.
- Weeks 7-8: full volume. Use the Mileage Increase Planner if rebuilding from significant time off.
Recurrence prevention: hold the rehab strength routine in your weekly schedule even after you feel 100%. The most common chronic-cycle pattern is dropping strength work the moment running feels normal again — and watching the pain return weeks or months later, often worse.
When to See a Doctor — and Which One
Most running knee pain resolves with the strategies above within 4-8 weeks. Seek medical evaluation if:
- Pain is severe (7+/10) or appeared suddenly during a run.
- The knee is swollen, warm, or locked — these suggest structural damage.
- Pain has not improved after 3-4 weeks of consistent strengthening and load management.
- Giving way or true instability — may indicate ligament involvement.
- Pain is constant at rest, not just with activity — may indicate inflammatory or systemic causes.
- Over 40 with new mechanical symptoms (catching, locking) — imaging may be warranted.
On who to see: a sports medicine physician or a physical therapist who actually treats runners is the right first stop. A non-sports orthopedic clinician whose only advice is "just stop running" is a dead end. As one physical therapist cautions about the language some clinicians use around imaging findings: "It's very evocative, and that can become very damaging because now patients are imagining every movement with that joint just grinding and grinding away. They stop moving, the pain gets worse." Sports medicine clinics give better triage; an MRI is rarely the first step and is most useful when 2-3 weeks of conservative management has failed.
Long-Term Knee Health for Runners
The hardest myth to kill is "running ruins your knees." It does the opposite. Alentorn-Geli et al. (2017) reviewed 17 studies covering more than 100,000 individuals and found recreational running was protective against hip and knee OA (3.5% vs. 10.2% in sedentary controls). The protection comes from cartilage conditioning under cyclical load, plus stronger supporting musculature.
Long-term knee health rules:
- Follow the 10% rule on volume — use the Mileage Increase Planner.
- Keep hip and quadriceps strength in your training year-round, not just when you're hurting.
- Watch training load with the Training Load Calculator.
- Allow real recovery between hard sessions — see the Rest Day Guide.
- Address pain early by modifying load, not by powering through until you can't run at all.
Sources & References
- (2016). 2016 Patellofemoral pain consensus statement from the 4th International Patellofemoral Pain Research Retreat. British Journal of Sports Medicine.
- (2019). Patellofemoral pain. Journal of Orthopaedic & Sports Physical Therapy.
- (2019). Risk factors associated with developing patellofemoral pain amongst runners. British Journal of Sports Medicine.
- (2014). Iliotibial band syndrome in runners: a systematic review. Sports Medicine.
- (2020). Soft tissue injuries simply need PEACE and LOVE. British Journal of Sports Medicine.
- (2017). The association of recreational and competitive running with hip and knee osteoarthritis: a systematic review and meta-analysis. Journal of Orthopaedic & Sports Physical Therapy.